Dental Products and Procedures FAQs in the Honolulu
At CBT, we are passionate about dental care and love sharing enlightening information about dental products and procedures in the Honolulu, as well as dentistry in general. Find answers to frequently asked questions about industry terms and what we offer.

Frequently Asked Questions
What Is a Human Tooth?
A tooth, bonelike in composition, is a specialized skin appendage consisting of calcium, other minerals, and protein polymers, with the function of supporting the oral cavity and human survival. Being rich in crystalline silica, teeth work like crystals or tuning forks to receive impulses from the internal and external environments.
A tooth is a sensory cutting or crushing tool given by our Great Parent God in our design as human beings. Teeth are used in speech, eating, building, and sensing the materials of the physical world. (Please avoid opening bottles and cutting thread, fish lines, or other things with one’s teeth!)
The tongue has the most perceptive sensory skin in our body and can distinguish two pinpoints less than a millimeter apart. Teeth and tongue work together in harmony, sensing the taste, texture, form, and heat/cold conditions of objects.
Children learn much about their physical environment by placing objects in their mouths. This method of research exploration aids greatly in intellectual development. The information gained from eye, ear, tooth, tongue, and hand exploration is critical to early childhood development. A majority of certain brain areas are connected with the oral-facial complex, more so than any other single limb or part of the body.
Therefore, as much as biologically possible, we must preserve our God-given health by retaining our teeth, as long as they are not decayed, diseased, or damaged.
What Is Tooth Decay?
Essentially, experts don’t know.
Fundamentally, tooth decay and bone decay are the same process occurring at different sites. Theories abound regarding the cause of decay. Experts may tell you how they “think” it happens but actually cannot identify the cause. CBT does not adhere to any of the theories being promulgated, for they all seem to presage a new vaccine, antibiotic, or chemical treatment to stop decay. The answer to dental decay is not a chemical element such as fluorine, a vaccine, or antibiotics.
These solutions may be contrary to good health because there are disadvantages to their use over a longer period of time.
Caries of the teeth, as in caries of the bone (periodontal disease), is no more than a “sweating out” of poisons, chemicals, or metabolites from inside our physical body. This is the principle of cleansing or purification, ejecting or scraping off internal pollutants.
A skin rash on your face, neck, arm, or abdomen is a normal cleaning process designed for your health by the Creator. For example, if one gets something in their eye, what happens? Immediately, the eye begins to water (washing out), and the lids blink (scraping off). This will continue until the object is cleared.
If you swallow something down your windpipe, what happens? You begin to cough until the object is ejected. The same is true with eating tainted food: poison in, poison out, vomiting, or diarrhea. If one looks, one will see this principle in action in all matters of bodily functions.
As noted previously, teeth and gums are skin in another form and place. And so, decay in this context is simply a “rash,” a release, or a leaking out of toxins. To further demonstrate this fact of life, recent reports from dental researchers showed that tooth decay was not necessarily a local phenomenon. That is, the “bacteria-acidogenic” theory of plaque action causing tooth decay was discredited.
Rats that were given sugar (a poison) directly into their stomachs, circumventing the teeth and avoiding any contact with the teeth, developed caries.
What Is a Root Canal?
This term refers to a common dental procedure in which the tooth area is treated to preserve the tooth structure rather than pulling it.
Within each tooth is a hollow space containing tissue that is similar to what one would find under the natural, healthy skin of the arm or other areas of the body. This tissue is called the dermis, and the skin is known as the epidermis. The tooth’s hollow space is called the “pulp chamber,” containing dermis-like tissue. The extension of this chamber into the roots is known as the “root canal.”
Unlike the tissue under the skin of the arm with its vast abundance of blood and nerve supply, the constriction of the roots of the tooth prohibits an abundant and easily reparable blood and nerve supply to the inside of the dental organ. Each tooth has its own nerve and blood supply and is thus considered an individual organ. The microscopic openings into the roots of the tooth decrease the ability of the tooth to recover from injury due to the paucity of reparative tissue.
So, when a tooth is impacted by a hard object, such as a water fountain or the handlebars of a bicycle, the tooth is separated slightly from its bone attachment and must reorganize the blood and nerve supply in order to recover. This recovery may not occur, for the severed blood supply may lead to the “pulp death” of the dental organ.
The death of tissue due to a loss of blood supply within a tooth is known as “gangrenous pulpitis.” If one had gangrene on the tip of the fingers due to frostbite, a surgeon would amputate the fingertips to preclude systemic blood poisoning.
But dentists are taught to “save the tooth” and hang on to the “housing,” the hard structure of the tooth, even though its contents are corrupt and necrotic. To save the tooth at all costs has become their mandate. We at CBT totally disagree with this obsolete teaching, for it goes against the principles of health and bodily hygiene.
Thus, in a traumatized tooth, nerves and blood vessels are constrained in their ability to readily flow and heal the damaged tissue. The tooth is, in a sense, much like a condenser or a mini filter, very slow in its ability to respond to trauma or the accumulation of systemic toxins. If the condensation of toxins or metabolites inside the tooth is greater than its capacity to carry them away from the pulp chamber, the tooth will die or “sweat the poisons out” through the dentin and enamel.
The blemishes occurring on the surface of the tooth, termed “dental decay” by the dental surgeon, is simply a “rash” or opening from the inside to the outside of the tooth for the purposes of purification. This makes sense to those who have studied the relationship of the dental organs, “odontons,” and organ systems, as delineated by Dr. Rheinhold Voll, the father of Bioenergetic Medicine.
The normal bodily response to dead tissue, waste material in or on the human body, is to send in bacteria to dispose of it. After the bacteria arrive, not as the cause of decay but as a result, the white blood cells of our immune system arrive. Both systems are there to keep things clean and to remove corruption from the tissues. As with a city dump, rats congregate and proliferate as a result of waste. The rats didn’t create the waste; the dumpsite did, and the rats, like the bacteria, are responding to the debris.
Given this understanding, we may realize that, from external trauma or internal trauma, the emission of toxins or metabolites from within the body through the dental organ (tooth) will cause irreversible damage to the tooth, necessitating its removal. In time, a dead tooth will be dissolved by the body’s natural clean-up processes and “pushed out” of its bone attachment. This is what is known as “periapical pathology,” a naturally occurring response to decaying matter, the tooth.
“Modern endodontics” (root canal therapy) attempts to save the once-living “housing” of the dental organ. This dead “housing,” or “dead tooth,” is a perfect nesting site for toxins and living entities, such as bacteria, fungi, viruses, and molds, since it is hollow and filled with billions of tubules. The remnant dead tooth cannot be sterilized in situ and thus acts as a focus of systemic infection for “endotoxemia.”
The latter condition is the circulation of poisons through our body due to periodontitis, more specifically in root canals as “apical periodontitis.” (In the late 1800s and early 1900s, Dr. Tilden wrote extensively about Toxemia, what we now identify 100 years later as “Endotoxemia.” His books are available at the Natural Hygiene Society.)
So, the upside of modern endodontics is that the patient keeps his dying or dead tooth, the endodontist keeps the money, and in a few years, the patient develops systemic conditions that the physician cannot resolve, and the source of the problem remains elusive.
The dentist has unknowingly created a site for “auto-infection” that is clearly related to blood vascular problems, diabetes, and arthritis, to name a few disabilities. Systemically, by allowing a “root cadaver procedure” to be done, the patient may develop a subclinical (not readily observable) systemic septic condition.
What the dentist accomplishes in a root canal procedure (endodontic procedure) is, at best, the removal of dead soft debris from the hollow space of the dental organ. It takes one or multiple appointments to do this. Each time, the dentist will “medicate” the pulp chamber and canals with highly toxic chemicals, such as sodium hypochlorite (bleach) or phenols, in an attempt to kill the vermin within. But this is akin to pouring perfume on a dead body!
As the doctor carries out this procedure, he will often prescribe antibiotics to abate pain, bleeding, swelling, fever, etc. This verifies what CBT has asserted for years, that the dead tooth has “apical periodontitis,” and it is only a matter of months or years before the tooth manifests systemic or local disabilities or both. These matters are not to be taken lightly and are contrary to a Bio-Logical approach. At CBT, we say, “If it’s dead, it should be out of your head!”
What Is a Dental Implant?
A dental implant consists of a metal or ceramic screw that is embedded in the jawbone where a tooth is missing.
Actually, anything foreign to the body, not available naturally in the original body as created by God, is an implant. A wooden sliver, metal shrapnel, a misplaced tack, or other object is technically an implant when inserted under the skin surface. The former are implants, for sure, but the generally accepted concept of implants is something that is placed by design into a human body for a specific purpose.
Tooth implants may work for a period of time, but our research indicates the ill-advisability of this new and generally unacceptable approach. Less than 6% of all dentists do this procedure, while it is reported that 80% of dentists suggest implants as a method of tooth replacement.
CBT has found that implants, like “root cadavers,” are foreign objects that are sooner or later rejected by a healthy human body. In all cases where implants were extracted, Hawaii Pathologists Laboratory reports indicated that the bone tissue next to the implant was composed of “dead bone,” “partially devitalized bone,” along with chronic and acute inflammation, fibrosis, granulomas, cysts, or abscesses.
Unfortunately, implants don’t work! Our advice is, “Don’t do it.” When the implants are surgically removed after swelling and infection set in due to the body’s rejection of this foreign object, the destruction of the jawbone is morbidly irreversible.
What Is a Crown or Cap?
The purpose of a “cap” or “crown” is to restore a badly broken-down or decayed tooth, with most or all of the enamel or dentin missing, returning it as much as possible to its normal form and function.
Crowns were developed when there was insufficient tooth structure remaining, and the dentist was unable to hang an amalgam filling inside the tooth. The solution was to wrap the tooth in gold. Prior to circa 1907, caps were pre-made “shell crowns.” Any metal could be used, but gold, due to its workability, was the metal of choice.
In 1907, Dr. Taggart presented a method of crown construction outside the mouth in an “indirect manner” that is still in use today. It is an accurate method, but it requires the wholesale removal of the outer covering and cuts deep within the dentin. When gold was used in the profession, conservative cutting of the tooth was taught and adhered to. But today, the tooth is generally rendered to a stub or peg.
When mercury (toxic) silver amalgam fillings are used, much of the tooth has to be reduced to hold the filling. It is the same with gold crowns, porcelain crowns, other modern crowns such as Targis Crowns, Ceramco Crowns, or other laboratory-fabricated crowns, which are made after an impression is taken of the tooth to be capped or crowned.
When all the enamel is removed, the tooth is very prone to death due to the loss of blood supply caused by operator-induced trauma. Death of tissue (tooth) due to loss of blood supply is gangrene.
In contrast, the new composites can be built around the tooth and smoothly adhere to the enamel and dentin by micromechanical and chemical bonding, thereby requiring minimal tooth reduction. A more bio-logical (life-logic) approach would be to restore the tooth with a restorative composite crown (RCC) created directly in the mouth. By so doing, one avoids radical cutting (reduction of the dental organ, the “enamel peel”) of the tooth.
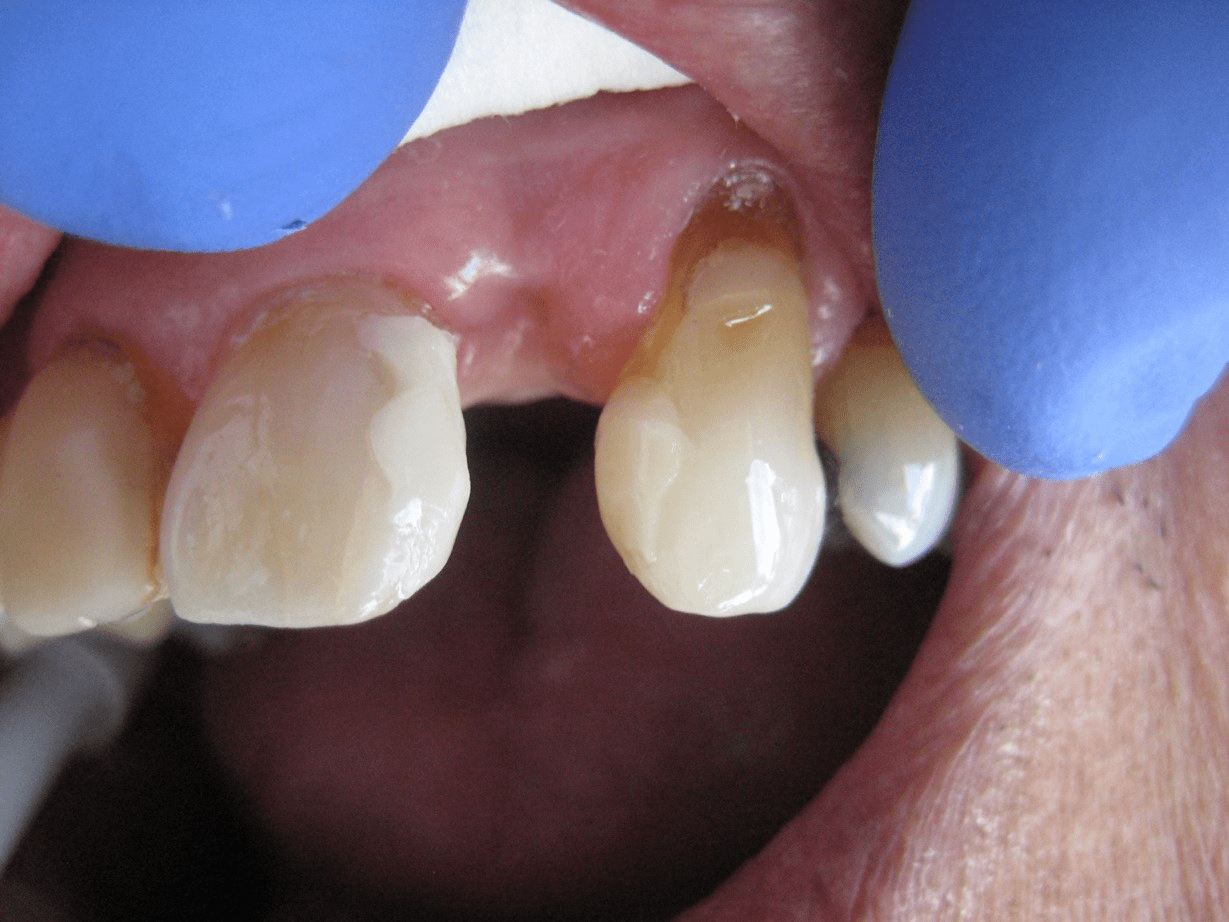
What Are My Alternatives If I Decide to Adopt a Bio-Logical Way, One Which Avoids Root
Canals, Implants, or Traditional Bridgework That, by Necessity, Requires the Enamel Peel?
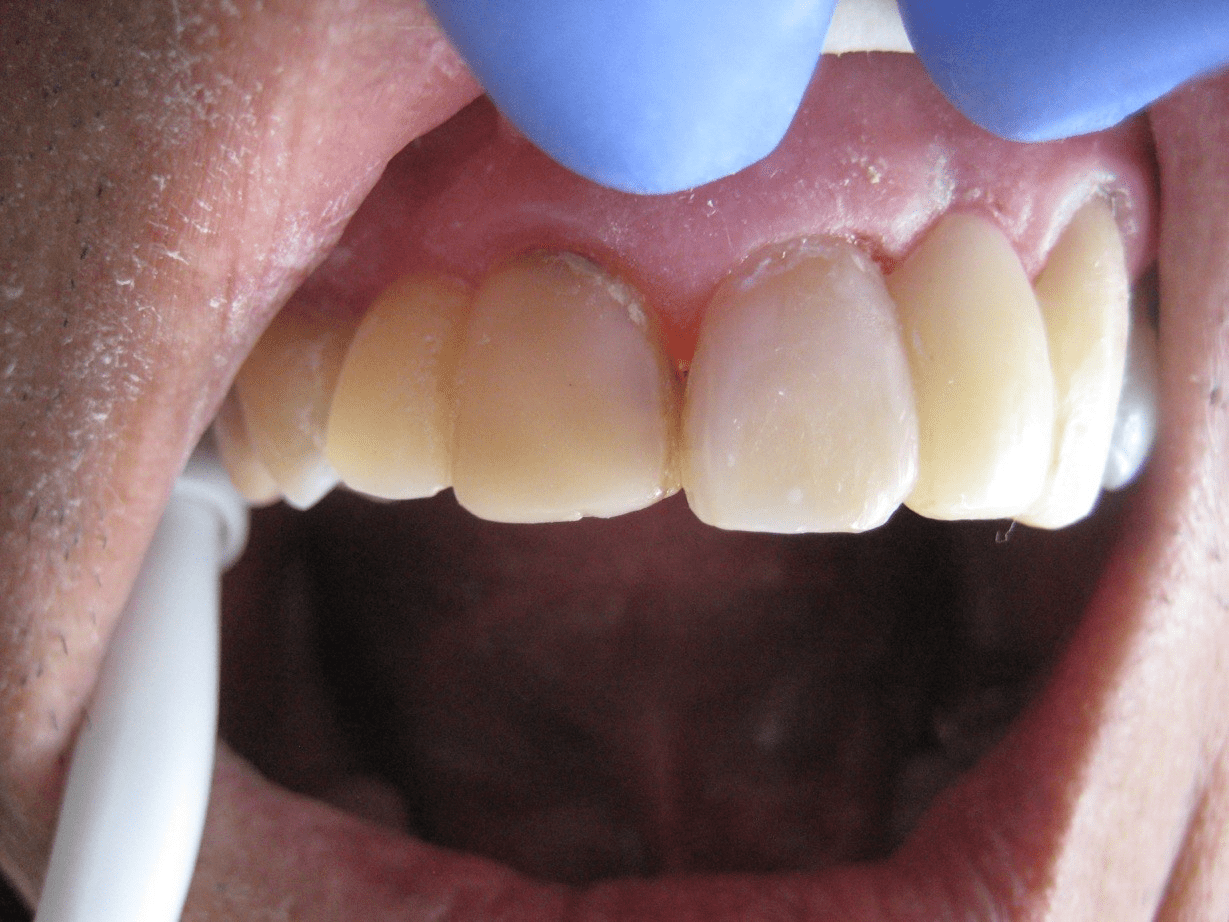
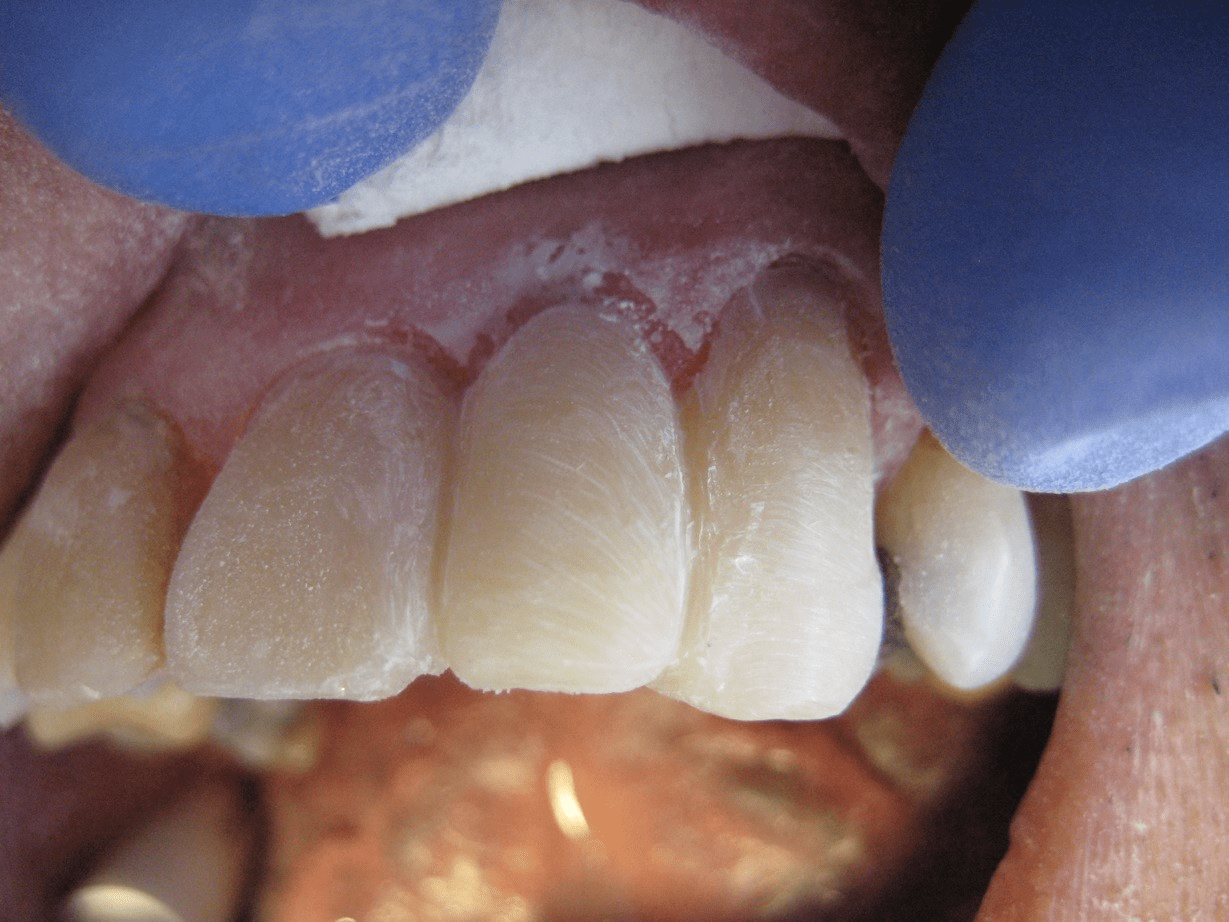
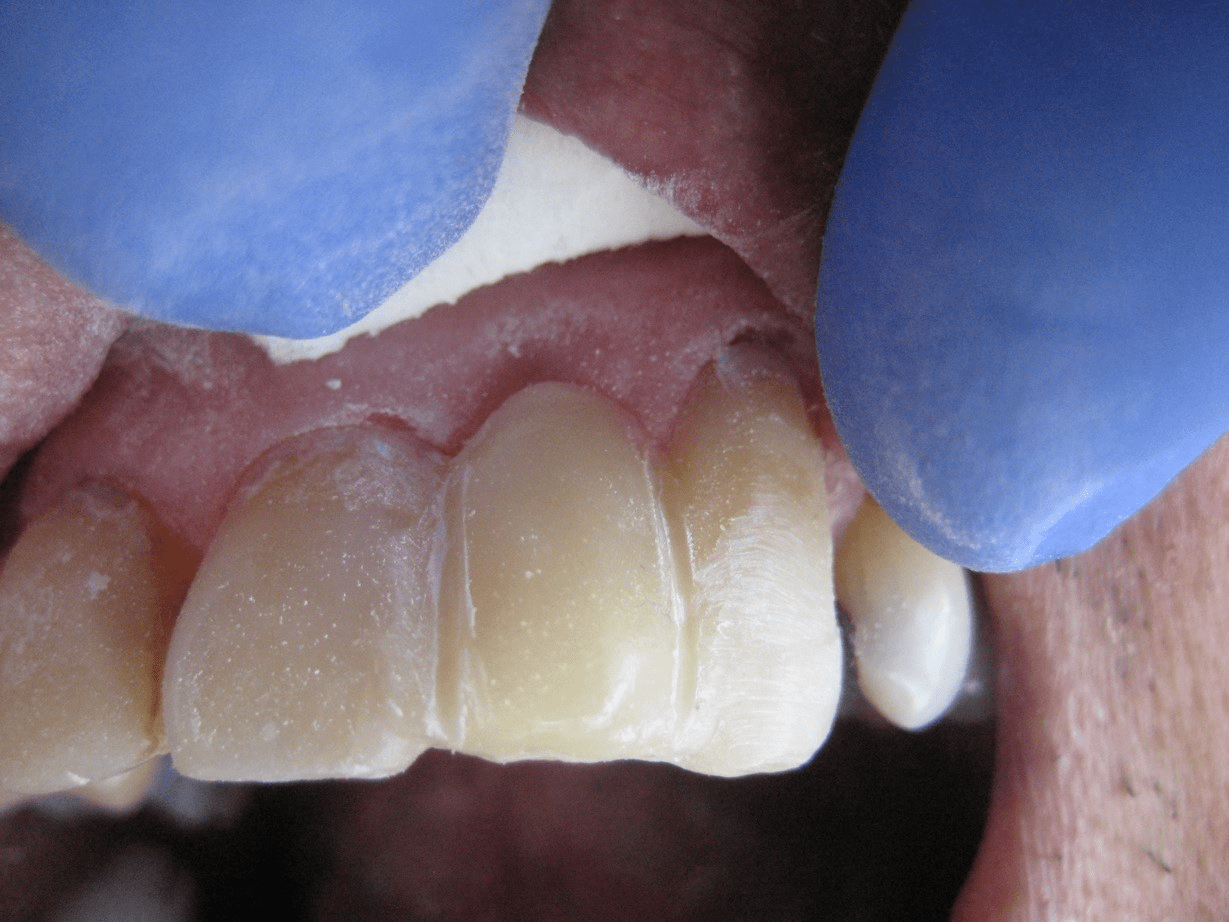
There’s a saying, “Simplify your life.” Take this opportunity to explore our photo series and captions. They will give you an idea of a method that you can try or your dentist can learn and adopt. The Carlson Bio-Logical Bridge™ is a possibility that may prove to be successful and highly satisfying.What Is the Carlson Bio-Logical Bridge™?
It is demonstrated in the photo essays by Dr. Carlson titled “Dental Artistry” and “Oral Sepsis,” and the pages describing the patent are available on this website, too. Fundamentally, the Carlson Bridge® (CB) and the Carlson Bio-Logical Bridge™ (CBB™) are innovative methods based on 23 years of composite use and 13 years of research and development of direct placement bridgework as an alternative to traditional or orthodox fixed bridgework that requires tooth-cutting.
CBB™ offers 1) no fiber or metal materials for strength; 2) one appointment; 3) no cutting of the teeth if teeth are without previous defects (fillings or crowns); 4) no anesthesia if the teeth are without defects; 5) tooth replacement immediately upon extraction (Here, anesthesia is recommended); 6) no laboratory procedures or costs; 7) direct patient input regarding shade, shape, and contour; 8) costs lower by 1/3 to 1/2 of traditional bridgework; and, 9) possibility to modify anytime in the future.
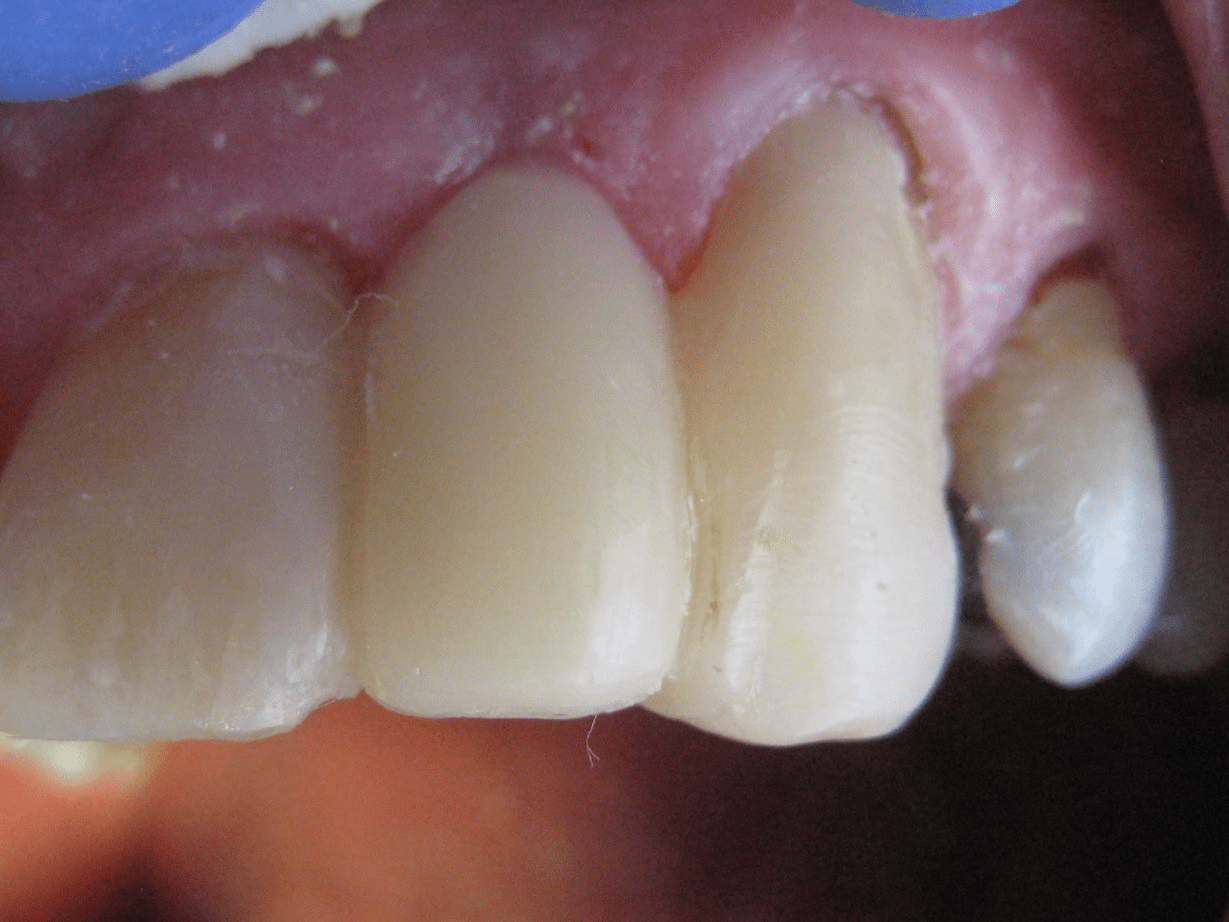
If the bridge, for some reason, should crack or chip, which is rare, it may be repaired quickly and directly in one’s mouth.
Dr. Carlson’s proprietary composite application and methodology ensures beauty, strength, durability, long life, and ease of bridge insertion. Dr. Carlson offers a three-day training in Honolulu for dentists and staff open to the bio-logical principle application in dentistry. He welcomes all inquiries from patients and doctors.
How Long Will the CBB™ Last Compared to Traditional Fixed or Removable Bridgework?
The bridge will last indefinitely with proper care and maintenance.
With over 200 Carlson Bio-Logical Bridges™ in use since 1989, we have found that a patient may expect the same or a greater life span as traditional fixed bridgework, either fixed or removable. Dental insurers have calculated, through their actuarial tables (statistical risks and life expectancies), that dental bridges (tooth replacements either fixed or removable) last, on average, three to five years.
Dental insurance will pay for a new bridge five years out from the date of construction and insertion. This is, we believe here at CBT, the most accurate assessment of the average life of a fixed or removable bridge, for at this five-year cut-off point, the insurance industry is protected from loss of profit. In about five years, 50% of dental bridges succumb to the trials and tribulations of one’s chewing, grinding, and eating habits. The other 50% may last decades.
If I Grind My Teeth, Will This Method Work?
Generally, yes. But grinding is an activity that is very detrimental to one’s teeth as far as wear is concerned. It should be understood that this factor may alter the longevity of the bridge and would be best addressed in a consultation prior to bridge insertion.
Grinding may be a result of jaw misalignment, psychological stress, or internal stress from poisons and electrical currents generated by mercury fillings or mixed metals used in dental procedures.
Is There Anything, Like Metal or Plastic, in the Composite Material That Could Cause an Allergic Reaction?
To our knowledge, no, not like the concentration of alloys in a full-metal bridge or a porcelain-fused-to-metal bridge. In full concentration, alloys have a galvanic effect, resulting in the corrosion of products.
The composite material is a non-metal, a plastic polymer, but does have aluminum silicates dispersed within the composition. The aluminum, in the form of aluminosilicates, does not corrode, and the material has no detectable direct current. The alumina is at the trace element level and does not pose a problem for human use, as far as we have been able to determine.
The CBB™ has no metal or any other structural components included in the bridge. The unique lamination process, which uses proprietary composite materials selected and applied according to meticulous procedural guidelines, limits allergic reactions. Our composite research, begun 44 years ago in 1980, has shown no allergic reactions to this date.
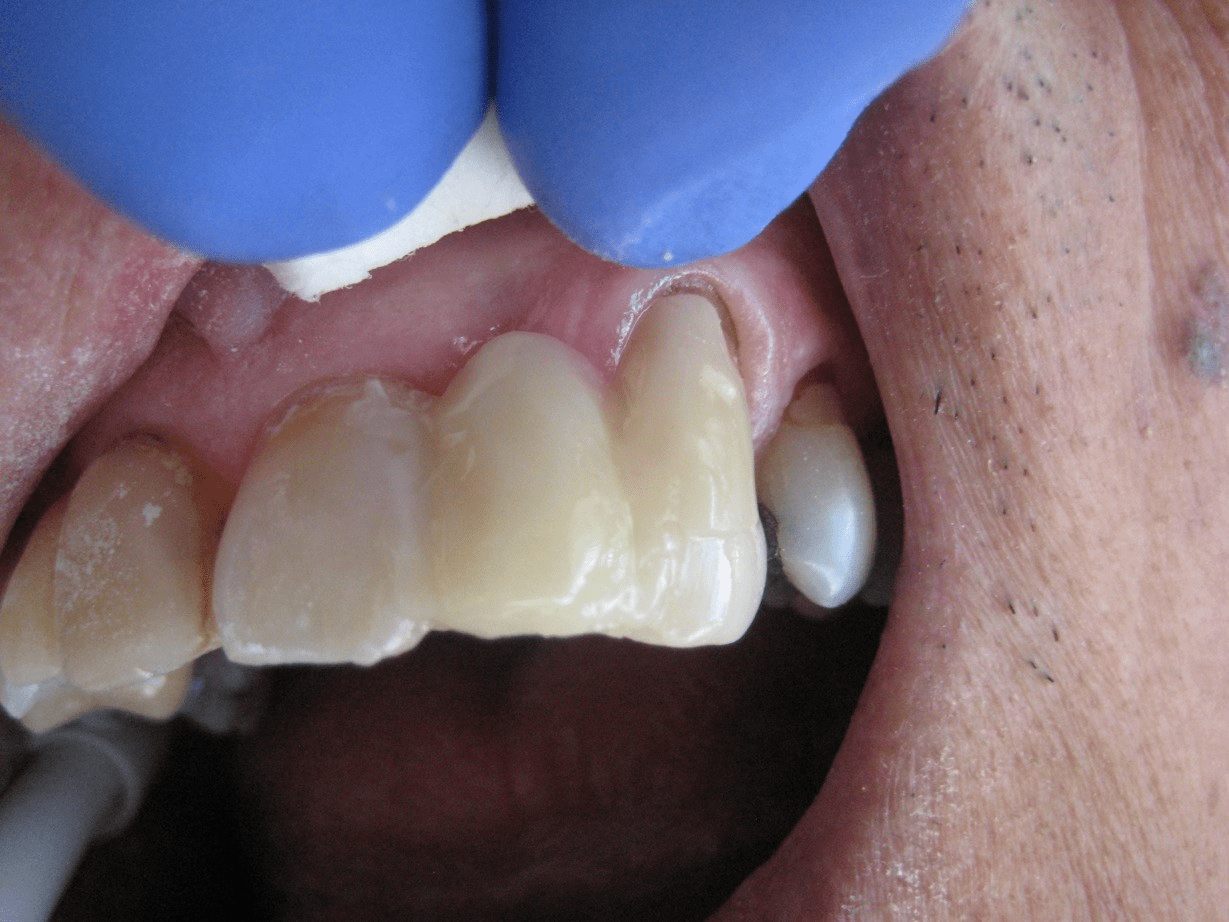
Does the “Blue-Green Thing” (Carlson Stent) Stay in My Mouth after the Bridge Is Completed?
No! The “blue-green thing” seen in our photos is an innovation not used in any other method of bridge fabrication. It is used only during bridge construction and uniquely forms the underside of the CBB™. After construction, it is removed effortlessly. This “blue-green thing” is the Carlson Stent, part of the patented process.
Is the Bridge Easy to Maintain and Clean?
Yes! You may brush and floss in the usual manner. Any toothpaste will work fine, but we strongly suggest un-fluoridated brands.
It is advisable to thread dental floss below the false tooth of the CBB™ and clean the underside of the bridge and the support teeth on either side once a day.
Actually, sea salt or baking soda in combination with sea salt is the best dentifrice known to man. Hawaiian salt is wonderful! Also, sea salt dissolved in warm water provides a gentler, healthier option than commercial mouthwashes, which may contain harmful chemicals, fluorine, alcohol, and dyes.
What Age Groups Will Benefit from This Approach?
All ages may benefit from this noninvasive, innovative alternative. From the youngster who has lost a front tooth due to a fall to the fellow who has endured the spaces left in the front of his mouth for years due to congenitally missing teeth to the senior who has lost teeth due to normal wear and tear, all may benefit. Our methodology is simple, clean, and effective — an idea whose time has come.
Will the Bridge Discolor with Time and Use?
No, it will not. Coffee, tea, nicotine, and alcohol use will not affect the composite. However, surface stains from these beverages or certain foods may occur. Proper brushing or professional dental cleaning easily removes stains. What works well for maintaining a bright and highly polished appearance is to buff the surfaces with a cotton tip applicator dipped in a slur of baking soda and sea salt.
Following our guidelines for daily hygiene, you can be assured of a healthy condition of gums and teeth, the minimization of offensive odors, and a dazzling smile.
Why Is This Method, the CBB™, More Biocompatible than Conventional Metal Bridges?
Conventional metal bridges contain concentrations of metals that may generate sufficient micro-currents and voltages of direct current, causing imbalances for the entire bio-electric-magnetic field, which is the pattern beyond the physical human body.
These subtle currents can be a source of disturbance for sensitive individuals. Small electrical currents may cause localized facial neuritis and neuralgia and, more broadly, may generate subclinical disturbances in distal tissue systems, organs such as the heart, liver, brain, spleen, pancreas, bowel, and stomach, and the musculoskeletal system.
These micro-currents act as “triggers,” throwing the body out of balance. Metal-containing bridges may have nickel, beryllium, copper, palladium, chromium, or other trace metals that electrolyze (corrode) and are absorbed into the body, causing allergic reactions such as gastritis, respiratory dysfunctions, arthritis, or other conditions.
The CBB™ is non-metallic, cannot corrode, does not require severely invasive tooth reduction (often none at all!), can be done without chemical injections, and provides optimal biocompatibility.
The composite materials used in our method are closest to that of the tooth structure’s chemical composition. These materials do not electrically disturb the energy channels of the body, also called the subtle “meridians” delineated in the ancient art and science of acupuncture and Oriental medicine.
How Many Appointments Are Necessary to Complete the Carlson Bio-Logical Bridge™?
Only one appointment, ranging from two to three hours, is needed to build the actual bridge. Preliminary consultation and follow-up appointments are advised to address any patient concerns, hygiene instructions, or minor corrections. Patients from out of state can schedule a short vacation in connection with their dental visit!
Can My Tooth Be Replaced Immediately after Extraction?
Yes! The Carlson Bio-Logical Bridge™ patented method is the only procedure that allows one to replace a tooth immediately after its removal. This is unheard of in conventional dentistry. Also, the nature of the procedure and materials affords the dentist the latitude to modify the bridge at any time in the future.
Can the CBB™ Be Damaged, and If So, What Should I Do?
The individual’s chewing habits, tooth grinding, and maintenance could be sufficiently damaging that the bridge breaks. The same could happen with conventional bridgework. Some patients have been known to snap metal bridges. Fractures, cracks, or separation from support teeth are easily repaired. Any dentist can learn this simple procedure or be instructed in bridge repair via electronic media.
Basically, the damaged area is cleaned and chemically treated, and new materials are applied according to Dr. Carlson’s procedures. All patients are advised to be aware of and modify their chewing habits before bridge construction.



Connect with Us for More Information
Contact the office at 808-735-0282 and leave a message, and we will reach out to you!